








- HOME
- INSTITUT PASTEUR DU CAMBODGE
- SERVICES
- Medical Biology Laboratory
- MBL - Our unit
- MBL – Information for Medical Professionals
- MBL - Analysis & Test Catalog
- MBL - List of transmitted analysis
- MBL - Sampling Manual
- MBL – Quality
- MBL-Prescription Sheet for General Testing
- MBL-Prescription Sheet for Microbiology
- MBL-Home Blood Sampling Appointment
- MBL - Information Sheets to fill out
- MBL - Instructions for Sample Collection
- Calibration Laboratory
- International Vaccination Center
- Laboratory of Environment & Food Safety
- Rabies Prevention Centers
- Rabies Serology for Pets International
- Voluntary Counseling & HIV Testing
- Medical Biology Laboratory
- RESEARCH UNITS
- PUBLICATIONS
- KEY STUDIES
- TEACHING
- JOIN US
- CONTACT US
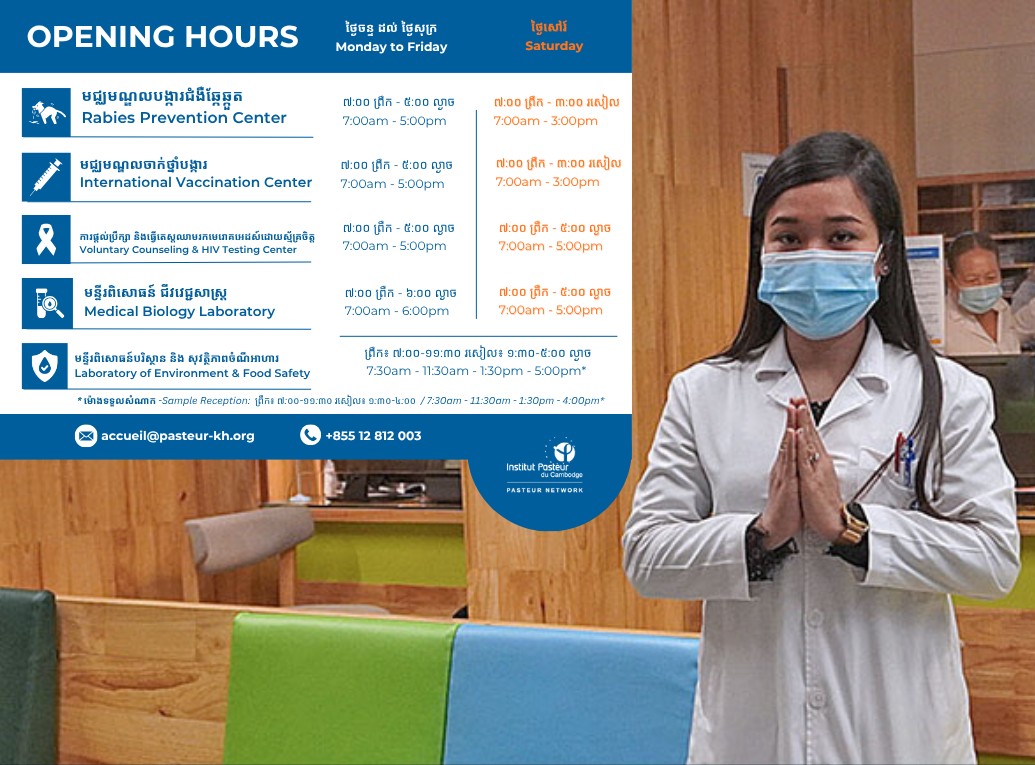
- OPENING HOURS
- SEARCH
Close
{kind=link}